Articles
Why Watching First Aid Videos Isn’t Enough in an Emergency
Videos can show the order of first aid clearly, but emergencies do not arrive with good lighting, quiet surroundings or a calm demonstrator. A person may collapse in a corridor, bleed heavily in a workshop or stop breathing while colleagues panic and phones ring.
The Gap Between Observation and Application
Watching a demonstration can make first aid feel familiar, yet familiarity is not the same as competence. In an emergency, the first aider must assess danger, make decisions, communicate with others and perform physical skills correctly. The gap between seeing and doing is most obvious in CPR, recovery position practice, bleeding control and defibrillator use. These skills need repetition, feedback and a realistic sense of how the body responds under strain.
The Illusion of Competence from Digital Media
A polished video removes the messiness of real incidents. The casualty is still, the camera angle is perfect and each action happens in order. Viewers may recognise the sequence and assume they can repeat it.
That confidence can disappear when the floor is hard, the space is tight and other people are asking what to do. Recognition helps, but it does not prove readiness.
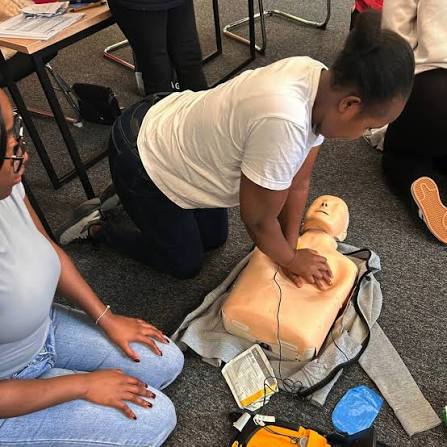
Missing the Physical Feedback of Manikin Practice
Manikin practice gives learners information a screen cannot provide. They feel chest resistance, body position, arm fatigue and the effort needed to keep compressions consistent.
That feedback often exposes errors quickly. A learner may believe they are pressing firmly enough, then discover their compressions are shallow, uneven or poorly positioned once an instructor observes them.
Understanding the Nuance of Compression Depth
CPR is not only about remembering a target depth or rate. Hand placement, straight arms, full recoil and steady rhythm all matter at the same time.
A video can describe these points, but physical practice teaches control. Learners feel how much force is needed and how quickly quality can drop when they become tired.
The Role of Muscle Memory in High-Stress Scenarios
Stress affects memory and judgement. People often fall back on actions they have physically rehearsed, rather than instructions they watched once.
Repeated practice builds a pattern: check, call for help, assess breathing, start compressions and communicate clearly. That pattern helps reduce hesitation when a real casualty needs immediate care.
Critical Limitations of Video-Only Learning
Critical Limitations of Video-Only Learning covers more ground than it first appears. The subsections below unpack Absence of Real-Time Instructor Correction, Inability to Replicate Emergency Stress Response, Common Errors That Videos Cannot Identify and The Importance of Peer-to-Peer Practical Drills, keeping the focus on what actually matters day to day for a team on the ground.
Video-only learning is passive. It cannot see the learner, correct unsafe technique or test whether they can perform a skill while thinking under pressure. Many first aid mistakes are not obvious to the person making them. Without supervised practice, errors can become habits, particularly in CPR, defibrillator use, recovery position practice and serious bleeding control.
Absence of Real-Time Instructor Correction
An instructor can spot bent arms, poor hand placement, leaning between compressions or unsafe movement when turning a casualty. Immediate correction matters because learners need to know what correct technique feels like.
Without that feedback, someone may copy the visible shape of a technique while missing the detail that makes it effective and safe.
Inability to Replicate Emergency Stress Response
A workplace emergency may involve noise, blood, machinery, distressed colleagues or a cramped room. A video cannot recreate that pressure or test how someone responds to competing demands.
Practical drills cannot fully reproduce a real emergency, but they can add urgency, movement and decision-making in a controlled setting. That makes hesitation visible.
Common Errors That Videos Cannot Identify
Videos can warn about common mistakes, but they cannot tell a learner they have just made one. Typical errors include shallow compressions, rushed breathing checks, loose bandages and poor defibrillator pad placement.
These errors may look small, yet they can affect care. Observation, repetition and correction are what turn general awareness into safer performance.
The Importance of Peer-to-Peer Practical Drills
Emergencies are social as well as clinical. First aiders often need to direct colleagues, reassure the casualty and ask someone to meet emergency services.
Peer drills help learners practise those instructions aloud. They reveal vague language, nervous silence and assumptions about who is doing what, before those problems appear in a real incident.
Why Practical Assessment is a Mandatory Requirement
Practical assessment exists because first aid competence has to be shown, not claimed. A person must demonstrate that they can carry out essential actions safely, in order and with suitable technique. For employers, this is especially important because first-aid arrangements should match workplace risks, staffing levels and likely incidents. Watching material can support learning, but it cannot confirm practical ability.
HSE Alignment and Workplace Compliance Standards
The Health and Safety Executive expects employers to assess first-aid needs by considering hazards, workforce size, working patterns and access to emergency medical services. HSE guidance is clear that arrangements should fit the workplace.
Recognised training supports that duty by giving first aiders supervised practice and a structured way to demonstrate practical capability.
Verifying Competence Through Hands-On Testing
Hands-on testing checks what a learner can do, not only what they can explain. CPR, bleeding control, recovery position practice and defibrillator use all require observation.
Assessment also checks sequencing. The right action done too late, or in the wrong order, can still leave a casualty at risk.
The Transition from Theory to Real-World Skill
Theory explains why a response matters. Practical work shows whether it can be delivered on the floor, beside a desk or near workplace hazards. Scenario practice helps learners make mistakes safely, receive feedback and repeat the skill with more control. That transition is where confidence becomes useful.
Ensuring Correct Use of Defibrillator Equipment
Defibrillators are designed to guide users, but practice still matters. Learners benefit from opening a trainer unit, placing pads correctly and responding to voice prompts.
That rehearsal reduces hesitation. It also reinforces safety, including keeping others clear during analysis and continuing CPR when instructed.
Bridging the Divide with Blended Training
Blended learning works best when each part has a clear purpose. Online materials can introduce signs, terminology and sequence before learners attend practical training. Classroom time can then focus on touch, repetition, correction and assessment. This approach respects the value of video without pretending it can replace supervised performance, especially where staff may need to act before emergency services arrive.
Combining Online Theory with Classroom practise
Online theory can cover the primary survey, shock, burns, seizures, reporting and the role of the first aider. Learners arrive with a basic framework already in place.
Classroom practice then becomes more active. Time can be spent kneeling, moving, compressing, bandaging, speaking and responding to scenarios.
Maximising Efficiency Through Hybrid Learning Models
Hybrid models can help employers plan training around shifts, departments and operational pressures while keeping the practical element intact. Efficiency should not become a shortcut. The hands-on session is the part that confirms whether knowledge has become usable skill, particularly for higher-risk environments.
Maintaining Knowledge with Regular Video Refresher
The HSE recommends annual refresher training for first aiders to help keep skills current. Short videos can support that habit between formal training points. They work best as reminders for trained people. CPR sequence, recovery position checks and recognition of time-critical conditions can all benefit from regular revision.
The Structure of a Professional Skills Assessment Day
A practical assessment day usually includes demonstration, supervised repetition, observation and feedback across key emergency responses. Learners may practise CPR on a manikin, use a trainer defibrillator and manage bleeding scenarios.
The aim is not performance for its own sake. It is to confirm that the learner can act safely when the situation demands it.
Ensuring True Preparedness for Emergencies
Preparedness means being able to move from recognition to action in the first few minutes. It does not mean diagnosing complex conditions or replacing clinical care. It means checking danger, assessing response and breathing, controlling serious bleeding, using available equipment and communicating clearly. For employers, it also means matching training and first-aid cover to real workplace risks, rather than assuming a video library is enough.
What “Ensuring True Preparedness for Emergencies” means in practice
What Ensuring True Preparedness for Emergencies means in practice covers more ground than it first appears. The subsections below unpack Key considerations for UK employers and Common mistakes and how to avoid them, keeping the focus on what actually matters day to day for a team on the ground.
Preparedness is visible. A first aider should be able to approach safely, speak to the casualty, call for help and begin appropriate care within the limits of their training.
It is also practical. Staff should know where the first-aid kit is kept, who the trained first aiders are and how to summon emergency help.
Key considerations for UK employers
Employers should start with a first-aid needs assessment and review it when work changes. New machinery, lone working, larger teams, different shift patterns or previous incidents may alter the level of cover needed.
Records also matter. Employers should know who is trained, when training expires and whether refresher activity is being maintained.
Common mistakes and how to avoid them
A common mistake is treating video completion as competence. Another is allowing trained staff to go too long without practical rehearsal. Employers can reduce risk by keeping equipment accessible, planning annual refreshers, checking first-aid cover across shifts and running short scenario drills where appropriate.
Conclusion
Videos have a useful place in first aid learning. They can explain sequence, show common signs and help trained people refresh knowledge between practical sessions. Their weakness is that they cannot observe the learner, correct technique or confirm safe performance.
Hands-on training remains essential because first aid is physical, pressured and time-sensitive. Learners need to feel compression depth, handle trainer defibrillators, practise casualty movement, communicate with others and make mistakes in a supervised setting before they face a real emergency.
For UK workplaces, the practical step is to review first-aid needs and check whether current cover still matches the risks. Video can support that process, but it should not replace recognised first aid courses that include assessed, face-to-face practice alongside clear supporting theory.Brity can help you find the right course.
Written by
William Hincks CEO Brity® First Aid

Why Watching First Aid Videos Isn’t Enough in an Emergency

History of Slot Machines Digital Entertainment for Everyone

Wet Dry Vacuums in Multi-Surface Cleaning: From Garages to Outdoor Spaces

Why Texas School Districts Are Prioritizing Acoustic Upgrades

Fortnite Cheats: Uncovering the Hidden Advantages

What Are The Biggest Challenges Faced By SAFe Scrum Masters In Large Enterprises?

How Braces Can Boost Professional Confidence and Entrepreneurial Success

Why Observability Tools Are Drowning Development Teams Instead of Helping Them

Video Production for Healthcare Brands: What Clinics Need to Know
Why Observability Tools Are Drowning Development Teams Instead of Helping Them

Emergency Electrician Near Me: What To Look Out For

Live-Dealer Streaming, Mobile-First Design, and the Evolution of Online Entertainment Platforms

Why Top Sellers Choose SpectrumBPO as Their Amazon PPC Agency for Sustainable Revenue Growth

Lumpsum Calculator: Plan Smarter, Grow Wealth Faster

The Real Key to Improving Your Pusoy Dos Online Skills on GameZone
How Braces Can Boost Professional Confidence and Entrepreneurial Success


Don Toliver Net Worth: Height, Age, Real Name, Career & More
Don Toliver is an American rapper and singer best known for his RIAA platinum certified songs, No Idea and After...


Finesse2tymes Net Worth: Height, Age, Real Name & Career
Finesse2tymes is an American rapper and recording artist. He is mainly recognized for his thunderous voice and motivational lyrics in...

Sugarhill Ddot Net Worth: Height, Age, Real Name & Career
Sugarhill Ddot is an American hip-hop recording artist best known for his songs, Real Facts and I Wanna Love You....


GloRilla Net Worth: Height, Age, Bio, Real Name & Career
GloRilla is an American rapper and hip-hop recording artist from Memphis. She is best known for her popular singles, “Westside...

Destroy Lonely Net Worth: Height, Age, Real Name & Career
Destroy Lonely is an American rapper best known for his 2022 mixtape, No Stylist. He is currently signed to rapper...
-
Rappers1 year ago
GloRilla Net Worth: Height, Age, Bio, Real Name & Career
-
 Businessman1 year ago
Businessman1 year agoBrandon Fugal Net Worth: How Rich is Skinwalker Ranch Owner?
-

 Rappers3 years ago
Rappers3 years agoBigXthaPlug Net Worth: Height, Age, Real Name & Career
-

 Businessman3 years ago
Businessman3 years ago7 Proven Lead Generation Strategies To Implement in 2023
-

 TV Stars1 year ago
TV Stars1 year agoKaleb Cooper Net Worth: How Rich is the TV Star Actually?
-

 News2 years ago
News2 years agoTrash To Treasure: Maximizing Space And Efficiency Through Junk Removal
-

 Internet Stars3 years ago
Internet Stars3 years agoMufti Menk Net Worth: How Rich is the Islamic Speaker Actually?
-

 TV Stars1 year ago
TV Stars1 year agoCarla Diab Net Worth: How Rich is the TV Star Actually in 2025?
You must be logged in to post a comment Login